Across the entire Australian population, there is limited research illustrating specifically the prevalence of hip pain. In 2003, however, Chen and colleagues (2003) concluded that general hip pain was reported in 39% of women from a 24’800 cohort.
From an anatomy point of view, the hip joint is a ball and socket joint. Due to the precise structure of the joint (large ball with a deep socket), the hip is able to withstand large repeated motions and the forces from weight bearing and movement. The demand on the hip joint from these large forces and movements place the joint at risk of developing various injuries.
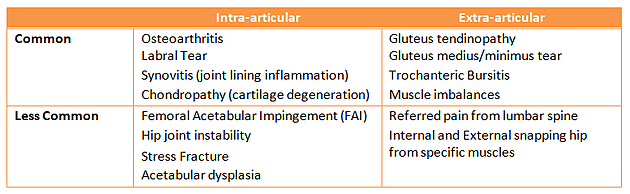
Disorders of the hip are generally categorised as intra-articular or extra-articular:
- Intra-articular: Driven by pathology, general wear and tear, or congenital reasons
- Extra-articular: Muscular/tendon origins of pain from strains, tears and overuse injuries
Imaging can assist in establishing a diagnosis, however, false positives (findings that may not be the precise source of symptoms) are common. Therefore, an accurate, comprehensive and efficient physical examination is important to determine the distinct pathology.
Different Conditions for Hip Pain
There are many different and broad diagnoses that can result in symptoms at, near or away from the hip joint. The following table illustrates the plethora of different diagnoses

The cause, symptoms, prognosis and treatment will differ based on the diagnoses above. The following sections will focus primarily on the more common diagnoses of hip-pain:
- Intra-articular: osteoarthritis and labral tear
- Extra-articular: gluteus medius tendinopathy and trochanteric bursitis
Osteoarthritis
Causes
Osteoarthritis, a condition that affects the bone, cartilage and ligaments of the whole joint is not caused by one sole factor, but by a combination of many risk factors such as previous hip injuries, jobs that have required climbing, squatting and heavy lifting, being overweigh and a family history of OA
Treatment
Exercise is one of the most important treatments as it reduces pain and maintains level of function. Low-impact activities are ideal and these can include cycling, walking and pool-based exercise. Specifically to pool-based exercise, the buoyancy of the water takes pressure off the hips allowing you to move more freely than on land.
Physiotherapy may include:
- Specific strengthening exercises for muscles around the hip
- Education and development of a self-management plan
- Gait and posture advice
- Taping
Labral Tear
Causes
The hip labrum has many functions including shock absorption, joint lubrication, pressure distribution and aiding in stability. In many cases, damage to the labrum has coincided with osteoarthritis. Other causes include trauma and sports injuries, having joint hypermobility and impingement pathologies.
Treatment
Physiotherapy may include:
- Improving neuromotor control via deep stabilisation muscle activation
- Gait and, if applicable, running retraining
- Return to sport plan, if applicable
Gluteus Medius Tendinopathy
Causes
Gluteal Tendinopathy (GT) is thought to be the primary cause of lateral hip pain. Many risk factors have been proposed for GT but few have been validated (Grimaldi, et al. 2015).
Risk factors include:
- Over 40 years of age
- Female
- Lower back pain
Symptoms generally arise from structural change at the gluteal tendons (connects muscle to bone) and bursae (fluid filled sacks that overly tendons and muscles). This process is thought to catalyse from a combination of:
- Recent increases in load- training for marathon, beginning gym again, or considerably increasing walking distance
- Prolonged period of insufficient load – poor muscle activation, low back pain may inhibit (turn off) this muscles ability to activate/li>
- Compression forces – from surrounding muscles, certain postures and stretches
Treatment
Physiotherapy can include (Grimaldi, et al. 2015):
- Education regarding posture and gait retraining
- Load management – reducing the catalytic process mentioned above
- Exercise therapy – Isometric, gentle loading exercise, and movement retraining
References
http://www.arthritisaustralia.com.au/images/stories/documents/info_sheets/2015/Condition%20specific/Osteoarthritis.pdf
Brukner, P. (2012). Brukner & Khan’s clinical sports medicine. North Ryde: McGraw-Hill.
Chen, J., Devine, A., Dick, I. M., Dhaliwal, S. S., & Prince, R. L. (2003). Prevalence of lower extremity pain and its association with functionality and quality of life in elderly women in Australia. The Journal of Rheumatology, 30(12), 2689-2693.
Grimaldi, A., & Fearon, A. (2015). Gluteal Tendinopathy: integrating pathomechanics and clinical features in its management. journal of orthopaedic & sports physical therapy, 45(11), 910-922.
Groh, M. M., & Herrera, J. (2009). A comprehensive review of hip labral tears. Current reviews in musculoskeletal medicine, 2(2), 105-117.
Magee, D. J. (2014). Orthopedic physical assessment. Elsevier Health Sciences.
Tibor, L. M., & Sekiya, J. K. (2008). Differential diagnosis of pain around the hip joint. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 24(12), 1407-1421.