Anterior knee pain is the most common presenting symptom to physiotherapy practices across Australia (Brukner & Khan, 2014).
In this blog:
- A basic anatomy of the knee is outlined
- Common causes of anterior knee pain are presented
- The evidenced based treatment of more common conditions are highlighted
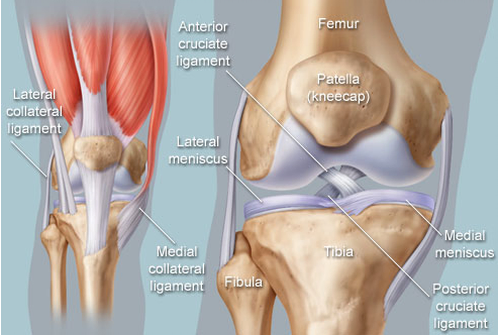
Anatomy of the Knee
The knee joint comprises of bones, ligaments and cartilage.
Medial = inner, Lateral = outer
- Bones: the thigh (femur), inside shin (tibia), outside shin (fibula) and knee cap (patella)
- Ligaments: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL)
- Cartilage: medial and lateral meniscus
Surrounding muscles can attach directly to the bones, ligaments or cartilage or indirectly via muscle fascia (connective tissue)

Known technically as a synovial hinge (likened to a door hinge) joint, the knee is a complex weight-bearing joint that is subject to high forces. This predisposes the knee and surrounding soft tissue to injury. Estimated forces through the knee are:
- Walking = 1.5 times body weight
- Single leg land in netball = 4 times body weight
- 1 metre jump = 25 times body weight
Different Conditions for Anterior Knee Pain

Many factors from the history of the complaint assist in a correct diagnosis. These include (among others) onset characteristics, specific location, and aggravating activity. See the table below for a comparison of these aforementioned features across more common conditions resulting in anterior knee pain:

Physiotherapy Management
Patellofemoral Joint Pain
Physiotherapy will involve exercise therapy and patient education in combination with foot orthoses, or patella taping. Exercise therapy, as concluded in high quality evidence (Cochrane), has been shown to be more effective than wait-and-see or placebo treatment (van der Heijden et al. 2015). Exercise therapy will result in reductions in pain and improve the functional level of the patient. Further, it may enhance long-term recovery, preventing the injury from arising again.
Infrapatella Fat Pad Irritation
An effective physiotherapy program targets the neuromuscular system in a weight bearing position – simply put, optimizing the way a patient moves. The program will not require any equipment, take no longer than 5 minutes, and be completed twice daily (McConnell, J. 2014). Pain reduction will be achieved with de-loaded taping of the fat pad (see picture below), with an initial aim to reduce pain when walking downstairs by 50%. The evidence proposes that, on average, 6 physiotherapy sessions over a 3-month period are required to overcome this condition (McConnell, J. 2014).


Infrapatella Fat Pad Deload Taping
Patella Tendinopathy
Exercise is the most investigated intervention for patellar tendinopathy. Previously, eccentric exercise in the form of an incline board squat (figure x) was suggested as gold standard for recovery. More recent research highlights the need for initial isometric exercise, as eccentric based exercises may be too aggressive. Below shows a continuum of specific exercises used throughout the rehabilitation.

Modified from Malliaras, P., Cook, J., Purdam, C., & Rio, E. (2015).
Pes Anserinus Tendinopathy
Current evidence concludes that physiotherapy is the mainstay in the treatment of pes anserinus syndrome (Rennie & Saifuddin, 2005). Initially this involves pain management strategies (ice), patient education and activity modification (Helfenstein Jr, M., & Kuromoto, J. 2010). After the pain and aggravating activities are controlled, specific exercises to activate, lengthen and/or strengthen muscle will be prescribed. Further research, however, is required to clearly define specific physiotherapy techniques beneficial in treating this pathology.
References:
Brukner, P. (2012). Brukner & Khan’s clinical sports medicine. North Ryde: McGraw-Hill.
Helfenstein Jr, M., & Kuromoto, J. (2010). Anserine syndrome. Revista brasileira de reumatologia, 50(3), 313-327.
Malliaras, P., Cook, J., Purdam, C., & Rio, E. (2015). Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. The Journal of orthopaedic and sports physical therapy, 1-33.
McConnell, J. 2014. Rescuing the Older Knee
Rennie, W. J., & Saifuddin, A. (2005). Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal radiology, 34(7), 395-398.
van der Heijden, R. A., Lankhorst, N. E., van Linschoten, R., Bierma-Zeinstra, S. M., & van Middelkoop, M. (2015). Exercise for treating patellofemoral pain syndrome. Cochrane Database Syst Rev, 1.