
Ankles injuries are the more common in indoor and court sports with higher incidence recorded in males 12 to 24 years and females above 30 years. lateral ankle injuries are more common than syndesmosis and medial ankle injuries.
Lateral Ankle Sprains
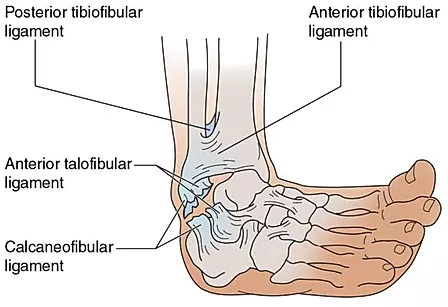
Lateral ligament sprains make up about 80% of all ankle sprains and are a very common presentation to physiotherapy clinics. Most of these injuries happen from a “rolled ankle” or inversion mechanism whereby the ankle is overstretched in a downward and inward direction. Factors such as the playing surface, awkward landing positions, opponent’s feet and sporting equipment can influence this injury.
Rehabilitation of lateral ankle sprains in the acute stages involves oedema (swelling) management, pain relief and to do no further harm to the injured area. The POLICE (Prevention of further injury, Optimal Load, Ice, Compression and Elevation) protocol is used usually used in the first 24-72hrs following ligament sprains.

Thereafter, more intensive physiotherapy may involve specific muscle strengthening exercises gentle range of motion to help promote healing and cellular repair and mobilization of painful or stiff joints.
Grades of ligament damage go from grade 1 (<10% fibres affected), Grade 2 (10-99% fibres affected) and grade 3 (complete rupture). Furthermore, the more severe the ankle injury may require immobilisation for a period of time before commencement of rehabilitation. Typically grade 1 injuries take 4 weeks to return to full sporting activities, grade 2 6 weeks and grade 3 10-12 weeks although each injury is different and the prognosis will vary.
Syndesmosis Injury
A syndesmosis injury or high ankle injury usually happens from an external rotation injury commonly from snowboarding accidents or contact sports such as rugby. It involves injury to the AITFL/ PITFL and/ or the “syndesmosis” or connection of the inferior (or distal) aspect of tibia and fibula. The syndesmosis is articulation where there is an interosseous membrane (a leather strap-like tissue) and interosseous ligament holding these bones in place. Rupture or separation of the syndesmosis rarely occurs by itself and more commonly occurs with other injuries such as fractures or other ligament sprains.

Taping or bracing high ankle sprains may be required to return to sport. Taping and/ or bracing allows the tape to tug on the skin firing certain receptors in your ankle to move it in a more preferable position and preventing excessive stretch on the vulnerable ligaments. Some individuals need taping or bracing 6 months after injury and some others feel they need it on all the time. Although the taping will help with function and returning to sporting performance even the best taping technique is no good without appropriate and diligent exercise rehabilitation which includes similar protocols to lateral ankle sprain.
Cuboid Syndrome
Cuboid Syndrome is defined as minor disruption or subluxation of the structural congruity of the calcaneocuboid portion of the mid-tarsal joint. Simply put, it is where the cuboid is out of place or losses its correct joint position. It is usually caused by plantarflexion/ inversion injuries or from overuse.

The plantarflexion/ inversion injuries are from forceful stretch or contraction on the lateral side of the ankle more specifically on the peroneus longus muscle. This powerful contraction causes a tug on the peroneal tendon which has attachments on the cuboid; hence the cuboid gets pulled out of its correct position. The other proposed mechanism occurs when repeated and chronic micro trauma causes an in directed effect on the cuboid causing subluxation. Although, previously thought to effect more individuals with flat feet (pes planus) a study by Marshall & Hamilton (1992) concluded that 17% of ballet dancers (who classically have high arches – pes cavus) had cuboid syndrome.
Treatments for cuboid syndrome are aimed at:
- Decreasing overactive muscles and spasm through massage
- Increased joint movement and decrease pain with joint mobilisation
- Improved biomechanics through strengthening foot intrinsic muscles
- Addressing imbalances and increasing proprioception with exercises and taping.
References
Bruckner, P & Khan, K. (2013). Clinical Sports Medicine. Elsevier Health.
Williams, D. S. Blaise; Taunton, Jack (2007). Foot and Lower Leg; Physical Therapies in Sport and Exercise. Elsevier Health Sciences.
Marshall, P. and Hamilton, W.G. (1992) Cuboid subluxation in ballet dancers. American Journal of Sports Medicine 20(2), 169-175.
Van Rijn, R. M., Van, A. G., Bernsen, R. M., Luijsterburg, P.A., Koes, B. W., Bierma-Zeinstra S. M. (2008) What is the clinical course of acute ankle sprains? A systematic literature review. American Journal of Medicine.
Neumann, D.A. (2002). Kinesiology of the musculoskeletal system. Foundation for physical rehabilitation.
Sman, A. D., Hiller, C. E., Refshauge, K. M. (2013). “Diagnostic accuracy of clinical tests for diagnosis of ankle syndesmosis injury: a systematic review”. British Journal of Sports Medicine.